| Human pregnancy | |
| ICD-10 | 00.-99. |
| ICD-9 | V22V22 |
| DiseasesDB | 10545 |
| MedlinePlus | 002398 |
| MeSH | D011247 |
Woman at 26 and 40 weeks of pregnancy Human embryo (8 weeks).
Human pregnancy
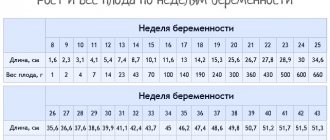
(lat. graviditas) - a special condition of a woman’s body in which a developing embryo or fetus is located in her reproductive organs. Pregnancy occurs as a result of the fusion of female and male reproductive cells in the fallopian tube, after which the formation of a zygote containing 46 chromosomes occurs. The sex of the unborn child depends on the set of sex chromosomes (XX or XY), while eggs always carry the X chromosome, and sperm carry the X or Y chromosome (in a 1:1 ratio). Thus, the sex of the unborn child is determined precisely by the sex chromosome, the carrier of which is the sperm (in the case of the X chromosome, a female child will be born, and in the case of the Y chromosome, a male child)[1]. As a result of cell division, a blastocyst is formed, which attaches to the wall of the uterus on the seventh day. In the first three months of pregnancy (first trimester), the fetal organs are formed, and by the end of the 12th week the placenta is fully formed. Through it, the fetus receives nutrients and the final products of metabolism are removed.
In obstetrics, a distinction is made between physiological and pathological pregnancy. Normally, any pregnancy ends with labor - a child is born, and in the case of a multiple pregnancy - twins (homozygous - identical or heterozygous - different). The duration of a non-pathological small pregnancy in a person is on average 38 weeks, which corresponds to 40 so-called obstetric weeks (which are counted not from the date of conception, but from the date of the last menstruation), however, even within the normal course, the periods can vary markedly from case to case.
Content
- 1 Planning pregnancy
- 2 Signs of pregnancy
- 3 Physiological pregnancy 3.1 Duration 3.1.1 Embryonic period
- 3.1.2 Fetal period
- 3.1.3 Physiological changes in the mother-fetus system
- 7.1 Smoking and pregnancy 7.1.1 Effect of smoking at different stages of pregnancy[13]
- 8.1 Classification
Planning a pregnancy
Main article: Family planning
Additional information: Symptothermal method and Contraception
Family planning
(English: family planning) is one of the main ways to solve the global demographic problem of stabilizing the Earth's population[2]. The most commonly used methods allow a couple to engage in satisfying sexual intercourse on a regular basis while reliably reducing the woman's chance of an unwanted pregnancy, at least until the couple decides that one should occur. Because of this, family planning includes methods that either prevent fertilization or act after fertilization to prevent implantation of the embryo.
Currently, there is an effective possibility of planning pregnancy. One of the most effective natural methods of family planning is the symptothermal method, but it is inferior to hormonal contraception in effectiveness and does not protect against sexually transmitted diseases like a condom.
When planning a pregnancy, it is important to determine the day of ovulation. After all, the point is that the egg (unfertilized) dies a day after ovulation, so the fertile period in the menstrual cycle begins 2-3 days before ovulation (sperm are active up to 3 days) and ends one or two days after ovulation. And the most favorable days for conception are the day before ovulation and the day of ovulation.
So, a surge in the level of luteinizing hormone means the beginning of the most favorable time for conception.
How to calculate the date of ovulation?
It's very hard to believe, but in every month there is only one day when it is possible to get pregnant . In very rare cases, this day occurs twice during the month.
There is a simple formula that can be used to calculate the day of ovulation without any assistance. Scientists have found that absolutely every woman ovulates 14 days before the start of her period .
If the menstrual cycle lasts 28 days, then it turns out that ovulation will occur on the 14th day after the last day of ovulation.
Agree, this calculation is very simple. However, there is one catch - this method is only suitable for those women who have a regular cycle . In addition, you can only calculate the day of ovulation if you have an accurate cycle schedule for at least six months.
Moreover, in individual cases, ovulation may occur a little earlier or a little later. But, if we take the expected date as the starting point, it turns out that pregnancy lasts 266 days (280-14=266) .
That is why doctors call a pregnancy that lasts from 266 to 294 days or from 38 to 42 weeks a normal full-term pregnancy.
When calculating, it is easy to notice that 280 days (40 weeks) are exactly 9 months .
However, obstetricians have their own month count. According to their calculations, pregnancy lasts 10 months . The fact is that the so-called lunar months, which consist of 28 days, are taken into account. This is exactly the period the cycle lasts for most women.
Signs of pregnancy
An increase in abdominal volume is one of the presumptive signs of pregnancy
Main article: Signs of pregnancy
Early diagnosis of pregnancy and determination of its duration is important not only from the point of view of obstetrics, but also due to the fact that anatomical, physiological and hormonal changes [3] that occur after conception can have a significant impact on the course of extragenital diseases that exist in history of the expectant mother. All signs that make it possible to diagnose pregnancy are divided into presumptive (doubtful), probable and reliable. They can be based on subjective or objective data[4]. However, nowadays, due to the widespread introduction of ultrasound diagnostics (ultrasound) into obstetric practice, the signs of pregnancy described in classic textbooks on gynecology and obstetrics are no longer so significant.
Doubtful (supposed) signs
(based on subjective data):
- vomiting or nausea (especially in the morning), changes in sense of smell, appetite or eating habits;
- emerging intolerance to certain odors;
- dysfunctions of the nervous system (drowsiness, lethargy, frequent mood swings, dizziness, malaise, irritability);
- frequent urination;
- engorgement of the mammary glands, their increased sensitivity;
- change (increase) in skin pigmentation (darkening) on the face, in the nipple area, along the white line of the abdomen;
- the appearance of pregnancy scars (striae) on the mammary glands, thighs, and abdominal skin;
- increase in abdominal volume.
Possible signs
(objective signs determined upon examination):
- sensation of fetal movement (in primiparous women at 18-20 weeks, in multiparous women - at 16-18 weeks);
- amenorrhea (lack of menstruation);
- enlargement of the mammary glands, appearance of colostrum;
- cyanosis (cyanosis) of the mucous membrane of the vagina and cervix;
- change in the shape, volume, consistency of the uterus (with internal obstetric examination);
- enlargement of the uterus from 5-6 weeks of gestation, first in the anteroposterior size, then in the transverse;
- Horwitz-Hegar symptom: softening of the uterus, especially in the isthmus area. During a two-handed examination, the fingers touch in the isthmus area without resistance. Characteristic for 6-8 weeks from the last menstruation;
- Snegirev's sign: variability in the consistency of the uterus: with mechanical stimulation or two-handed examination, the uterus thickens and contracts, then becomes soft again.
- Piskacek's sign: in the early stages, asymmetry of the uterus is observed, protrusion of one of the corners where implantation took place. It disappears with increasing time.
- Gubarev and Gauss sign: in the early stages there is slight mobility of the cervix, which is associated with significant softening of the isthmus.
- Genter's sign: in the early stages, due to softening of the isthmus, there is an inflection of the uterus in the front and a comb-like thickening on the anterior surface of the uterus along the midline (not always determined);
- Express pregnancy test.
Reliable (undoubted) signs
(detected in the second half of pregnancy):
- the fetal heartbeat is determined (using an obstetric stethoscope, you can listen to the fetal heartbeat);
- detection and palpation of large (head, pelvis) and small (arms, legs) parts of the fetus and/or its movements (starting from the second trimester of pregnancy) during an external obstetric examination. When palpating the abdomen using Leopold's maneuvers (external obstetric examination techniques), the position, position, appearance, presentation of the fetus and the relationship of the presenting part to the pelvis are determined;
- the fetal skeleton is determined on an x-ray and echogram;
- determination of the fetus and placenta using ultrasound diagnostics.
Physiological pregnancy and accompanying changes in the body
Pregnancy
is a physiological process of development in the female body of a fertilized egg, beginning from the moment of fertilization of an egg matured in the ovary (female reproductive cell) by a sperm (male reproductive cell).
Physiological pregnancy lasts on average 10 lunar months (1 lunar month – 28 days), i.e. 40 weeks or 280 days. The entire pregnancy period is usually divided into trimesters. The 1st trimester begins with fertilization and ends at 12-13 weeks, the second ends at 28 weeks, and from the same period begins the third trimester of pregnancy, ending with childbirth.
Fertilization usually occurs in the ampullary portion of the fallopian tube facing the ovary. Thanks to the rhythmic contractions of the fallopian tubes, the fertilized egg moves into the uterine cavity. During this movement along the fallopian tube, the egg turns into a multicellular embryo (fertilized egg), densely covered with delicate villi - with their help it attaches to the mucous membrane lining the inner surface of the uterus. From the moment of attachment to the mucous membrane of the uterus, the formation of first the embryo, then the fetus begins, accompanied by a restructuring of all functions and systems of the woman’s body. At the site of attachment of the embryo, the villi grow luxuriantly and form the so-called baby's place or placenta, connected to the fetus through the umbilical cord. Through the placenta, nutrients and oxygen are supplied to the fetus from the mother through the blood vessels of the umbilical cord, and metabolic products are removed. Functional changes in the body of a pregnant woman are essentially adaptive reactions that provide favorable conditions for the development of the fetus.
Diagnosis of early pregnancy.
The possibility of pregnancy can and should be assumed in any woman of childbearing age who has not had her period on time or who has amenorrhea (absence of menstruation) during regular sexual activity.
Thus, the first sign of pregnancy is usually the absence of menstruation at the scheduled time
.
A few days after the onset of menstruation, most women experience nausea and even vomiting. Vomiting usually occurs once or twice a day, in the morning, immediately after getting out of bed, but it is not so severe as to cause noticeable metabolic disturbances. Increased urination
is also common in non-pregnant women during the premenstrual phase.
However, in pregnant women it is more noticeable and can give the first indication that conception has occurred. Changes in the mammary glands
are also noted from the very beginning of pregnancy and are especially noticeable in women who are pregnant for the first time.
Usually a woman feels some stretching of the mammary glands and their soreness. The swollen mouths of the areola glands around the nipple can protrude upward, forming the so-called Montgomery tubercles. With sufficient lighting, the swelling of the superficial veins, especially those around the nipple, becomes visible. The breast loses its usual softness and strands of swollen glandular ducts can be felt in it, running from the periphery to the nipple like spokes in a wheel. After 14 weeks, nipple discharge appears, progressing as pregnancy progresses, and the mammary glands noticeably increase in size. After 16 weeks, pigmentation of the nipple
, especially pronounced in dark-skinned women.
From about 12 weeks, and in thin women a little earlier, you can feel the fundus of the uterus through the anterior abdominal wall, which at 20 weeks approaches the lower edge of the navel, and at 36 - to the xiphoid process of the sternum.
Multipregnant women notice fetal movements earlier
than first-time pregnant women. The former usually notice movements between 16 and 18 weeks, and the latter between 19 and 21. Data about these sensations can be very important for determining the duration of pregnancy and the upcoming birth, so the woman should try to more accurately remember the date of the appearance of fetal movements.
There are also special methods for diagnosing pregnancy. In doubtful cases, a woman can determine the onset of pregnancy using express pregnancy tests
, sold in pharmacies or by conducting an immunological test in a antenatal clinic to determine the hormone - human chorionic gonadotropin.
Modern diagnostic ultrasound devices make it possible to establish pregnancy at a minimum period of 2-3 weeks.
The accuracy of diagnosis increases with dynamic observation and transvaginal scanning (when a special sensor is inserted into the vaginal lumen and the examination is carried out as if from the inside).
Every pregnant woman must register with the antenatal clinic
and the sooner the better. After all, in the early stages of pregnancy, she still remembers exactly the days of her last menstruation, and the accuracy of the information can be checked during a bimanual examination performed by a gynecologist. In addition, during this period, the doctor needs to obtain initial data on pulse rate, blood pressure, blood hemoglobin level, body weight, so that if they change at a later date, he can quickly assess the situation and, if necessary, take the necessary measures without delay . It is during this period that the doctor needs to identify concomitant diseases of the internal organs, such as hypertension or heart disease, peptic ulcer disease or diabetes mellitus, which ultimately can have a significant impact on the condition of the expectant mother and her child and modify the management of the pregnant woman accordingly.
In addition, the primary medical examination includes determination of blood group, Rh factor, as well as serological tests for syphilis and HIV infection.
If the woman is 35 years or older
, that is, the risk of chromosomal abnormalities that can lead to the development of various fetal malformations and diseases (the most common is Down's disease). In these cases, the doctor will recommend undergoing a special examination - amniocentesis (a thin needle is used to puncture the wall of the uterus and amniotic sac, and the resulting amniotic fluid is analyzed). In addition, women undergo ultrasound examination (ultrasound), which is acceptable at any time (its harmlessness has been confirmed by numerous studies conducted for more than 30 years all over the world).
In general, pregnancy can be considered as a process of long-term physical adaptation of the mother’s body, necessary to meet the needs of the growing fetus and ensure the constancy of the internal environment in which its growth occurs. The degree of this adaptation generally exceeds the needs of the fetus, so there are significant reserves to endure periods of stress or deprivation without significant changes in the fetal environment. Each of the systems of a woman’s body undergoes serious changes and tests. For example, by 34 weeks of pregnancy
the amount of circulating blood increases by 30-40% and then decreases slightly. The level of blood proteins decreases from 7 to 6 g/l, which causes a drop in plasma osmotic pressure, due to which pregnant women are prone to edema. The total number of leukocytes (white blood cells) increases slightly, but the ESR (erythrocyte sedimentation rate) in pregnant women increases sharply and can reach 50 mm/hour. The platelet count approximately doubles. The lipid content in the blood increases from 6 to 9 g/l, mainly due to cholesterol.
Mean arterial pressure, apart from a tendency to drop slightly in mid-pregnancy, increases slightly, which facilitates the transfer of oxygen from mother to fetus. Oxygen consumption increases. Speaking about changes in the vascular system, we note that pregnant women experience dilation of skin vessels, as a result of which the woman feels the cold less and can sometimes feel worse in hot weather. The increase in superficial blood flow is more noticeable on the ulnar side of the palms as palmar erythema (redness).
As pregnancy progresses, the movement of the diaphragm is significantly limited and breathing becomes more thoracic in nature. The volume of respiratory air increases, which reduces the pressure of carbon dioxide and thus facilitates the excretion of carbon dioxide through the placenta. By the time of birth, oxygen consumption increases from 10 to cm3. in a minute.
In the first and second trimesters of pregnancy
renal blood flow increases, gradually returning to its original level at the time of delivery. The rate of renal filtration (urine production) increases by 50%, returning to normal only after childbirth. The excretion of urea and uric acid also increases. At approximately 16-20 weeks of pregnancy, the renal threshold for filtering glucose drops sharply, which is why glucosuria (sugar in the urine) occurs quite often in pregnant women.
The weight gain of a pregnant woman varies widely from person to person, but on average a woman gains 12 kg during pregnancy.
. One third of the gain, 4 kg, is gained in the first half of pregnancy, and the remaining 2/3 (8 kg) in the second. 60% of the total body weight gain is due to fluid retention, which in turn is caused by the accumulation of sodium (about 20 g) due to increased secretion of the hormone aldosterone. The retained water is distributed as follows: in the blood plasma 1.3 l; in the fetus, placenta and amniotic fluid – 2 l; in the uterus and mammary glands - 0.7 l and in extragenital interstitial fluid - 2.5 l. At the time of birth, the fetus, placenta and amniotic fluid together weigh about 5.5 kg. And this mass is lost after childbirth. The remaining 6.5 kg is due to the uterus, breast enlargement, extragenital fluid retention (increased blood volume, edematous fluid, etc.) and fat reserves, especially in the thighs and buttocks. After a sharp decrease in body weight in the first four days after birth due to increased diuresis resulting from the cessation of placental hormones, it continues to gradually decrease over the next 3 months or so.
Pregnant women also experience increased skin pigmentation
, especially pronounced on the face, around the nipples and the white line of the abdomen (brighter in brunettes compared to blondes). This phenomenon is caused by an increase in the amount of circulating melanocyte-stimulating hormone. Longitudinal stripes (striae of pregnancy) 5-6 cm long and about 0.5 cm wide appear on the stomach and thighs. At first they are pink, but then they become pale and slightly denser.
Birthmarks appear in more than 50% of pregnant women. The intensity of the sebaceous and sweat glands during pregnancy increases.
To summarize, we can say that during the gestational period, profound shifts in physiological functions occur, aimed at meeting the needs of the developing fetus and compensating for the physical changes in the mother’s body that are caused by these shifts. At each stage of pregnancy, physiological changes are aimed at meeting the needs of the fetus and providing such reserves that allow it to grow and develop continuously.
Although it is rightly believed that pregnancy is a physiological state of the body and many women are ready for a harmonious relationship with their unborn child, it is known that pregnancy is also a period of tension and stress and that in few women it occurs without functional or organic disorders of varying degrees of severity.
Make an appointment with specialists by calling a single call center:
+7(495)636-29-46 (metro stations “Schukinskaya” and “Street 1905 Goda”). You can also make an appointment with a doctor on our website, we will call you back!
Pregnancy is physiological
As with any pregnancy, its occurrence is associated with the process of fertilization (conception), that is, the fusion of a mature male reproductive cell (or gamete), called a sperm, and an egg, a female reproductive cell (or gamete). Thus, the common cell (zygote) formed upon completion of the process of fertilization or fusion of two gametes is the beginning of a new organism [1].
Duration
Main article: Course of pregnancy in humans
The average length of pregnancy from fertilization to birth is 38 weeks (embryonic period). The average duration of pregnancy from the beginning of the last menstrual period to delivery is 40 weeks (obstetric period). The use of obstetric dates is more common in medicine, since the date of fertilization is usually difficult to determine.
Dating of pregnancy in weeks and months from the date of the last menstruation
Human intrauterine development is usually divided into periods. The development of the embryo from fertilization of the egg to the beginning of implantation (the first week of development) is characterized as the preimplantation period (see Conception in humans), subsequent development is referred to as the postimplantation period. During the preimplantation period, the embryo is not attached to the wall of the mother’s uterus; during the first 4 days, the embryo moves from the site of fertilization (ampullary part of the fallopian tube) along the fallopian tube towards the uterus; on the 5-6th day of development, the embryo is in the woman’s uterus, preparing itself for implantation ( see Zona pellucida). It is also customary to isolate embryonic
(the first 8 weeks from fertilization) and
fetal
(from the 9th week before birth) periods of development. During the embryonic period, the spatial organization of primary structures (morphogenesis), the initial differentiation of cells and the formation of organ systems (organogenesis) occur. During the fetal period, organs develop within the framework of the formed systems, and the size of the fetus increases to a significant extent.
Embryonic period
Initial stages of human embryogenesis.
Main article: Embryonic period
The embryonic period lasts from the moment of fertilization until the end of the 8th week of the embryonic period (10th week of the obstetric period). During the embryonic period, human embryogenesis occurs, in particular, processes such as fertilization, cleavage (formation of multicellularity), implantation (introduction into the uterus), gastrulation (formation of germ layers), histogenesis (tissue formation), organogenesis (organ formation), placentation and other processes. During the embryonic period, the embryo increases in size from 0.1 mm (fertilized egg) to 3 cm (excluding membranes). Initially, the embryo does not resemble a baby, and only gradually does it acquire features and structure similar to a baby. In the last week of the embryonic period, some embryonic structures disappear (gill arches and gill slits, tail, allantois decreases).
Fetal period
Main article: Fetal period
The fetal period lasts from the 11th week of obstetrics until birth. By the beginning of the fetal period, all organ systems of the fetus are formed (development occurs within the framework of the formed systems), externally the fetus resembles a baby, intensive fetal growth and a change in body proportions occur.
The shorter the gestational age, the higher the sensitivity of the embryo and fetus to negative influences. During the embryonic period, the risk of spontaneous abortion is approximately 10 times higher than during the fetal period.
A woman’s pregnancy is usually divided into so-called “trimesters” (periods of three months). Accordingly, they talk about the first, second and third trimesters of pregnancy. Each trimester is characterized by certain obstetric features and risks.
- 4 weeks after conception[5]
- 8 weeks after conception[6]
- 18 weeks after conception[7]
- 38 weeks after conception[8]
- Relative size in 1st month (simplified image)
- Relative size in 3rd month (simplified image)
- Relative size at 5th month (simplified image)
- Relative size in 9th month (simplified image)
Physiological changes in the mother-fetus system
More information: Immunobiology of pregnancy
From the moment pregnancy occurs, two very closely interconnected systems are formed:
- functional system of the maternal body, which ensures the creation of all conditions necessary for the proper development of the fetus and
- the functional system of the fetus, primarily responsible for maintaining its normal homeostasis.
The main link between these two functional systems at a certain stage of pregnancy becomes the placenta - thus, to protect the foreign (from the point of view of the mother’s immune system) fetus, a feto-placental barrier is formed. Due to the presence of a close morphofunctional connection between the fetus and the placenta, both of these formations are usually described as a single fetoplacental system [1].
Pregnancy too long
Causes
Many expectant mothers are more afraid of a premature pregnancy than a post-term pregnancy. However, in fact, post-term pregnancy is very dangerous .
Doctors still cannot give an exact answer as to what is the reason for pregnancy being too long. It is customary to distinguish two factors of postmaturity - medical and psychological .
From a medical point of view, the cause of the problem lies in the woman’s physical unpreparedness for childbirth.
This can be explained by the following factors :
- late cervical ripening;
- muscular disorders of the uterus and myometrium;
- slow fetal development;
- hormonal problems;
- endocrine and gynecological diseases of women;
- pathology of the uterus;
- heredity.
Moreover, the duration of pregnancy also depends on the age of the mother . Most often it is carried to term during the first late pregnancy .
All causes that can be attributed to a medical aspect are identified through additional examinations . But the psychological side is quite difficult to identify.
It happens that psychologically a woman is not at all ready for childbirth . The reason for this is an unconscious fear of the birth process. A woman may fear pain or the possibility of losing the baby, slowing down the onset of the natural process.
At the first signs of post-maturity, you should consult a doctor. By performing an additional ultrasound, the specialist will be able to determine the condition of the placenta, amniotic fluid and, of course, the child.
When, after an ultrasound, traces of meconium are found in the amniotic fluid or problems with the baby’s heartbeat are detected , then, in this case, the doctor will definitely prescribe induction of labor or a cesarean section.
These appointments should never be refused, because the consequences of a post-term pregnancy can be disastrous.
Perinatal diagnosis
Main article: Prenatal diagnosis
Perinatal diagnosis
— prenatal diagnosis of developmental pathologies — is carried out in several stages. Between the 10th and 13th weeks, perinatal screening for the risk of Down syndrome and Edwards syndrome is carried out using ultrasound and biochemical markers. The period between the 16th and 18th weeks is considered the optimal period for conducting the so-called triple biochemical screening for Down syndrome, Edwards syndrome and neural tube defects. Triple screening can be done from 14 to 20 weeks.
The first sensation of fetal movement usually occurs at 18 weeks in multiparous women and 20 weeks in primiparous women. However, there may be strong variability over several weeks. Thin women, as a rule, begin to feel movements earlier than plump ones.
At 20-24 weeks, a repeat ultrasound is performed to determine the condition of the fetus by organs.
At the 24th week, if indicated, a Doppler study of the blood flow of the placenta is performed to exclude the risk of developing placental insufficiency; at the 26th week, a glucose tolerance test is performed to exclude the risk of gestational diabetes.
At the 28th week for a multiple pregnancy and at the 30th week for a singleton pregnancy, prenatal leave is prescribed and an exchange card is issued, which from this day on you must take with you everywhere.
At 30-34 weeks, a third ultrasound is performed to determine the condition of the fetus and placenta.
After 37 weeks, the pregnancy is considered full-term. Normally, childbirth takes place at the 40th week, although less than 5% of women give birth according to an accurately calculated period, and variability of 2 weeks in both directions is considered normal. Pregnancy lasting more than 42 weeks is considered post-term.
- Play media file
3D ultrasound - fetal movement at 12 weeks
- 75mm fetus (about 14 weeks)
- Fetus at 17 weeks
- Fetus at 20 weeks
How many weeks are boys born?
“At what week of pregnancy do they give birth to boys?” – this is a burning question many parents ask. There is an opinion that boys are born several weeks later than expected (38-42 weeks of pregnancy). As statistical data show, there is no specific pattern between the gender of the child and the date of his birth.
It all depends on the development of the pregnancy itself, the woman’s constitution, hereditary and other factors. And even more so, it is impossible to change the gender of an already conceived child, because gender is determined at the moment of conception. Therefore, if there is an urgent question regarding the sex of the baby, then it is better to resort to artificial insemination.
Pregnancy is pathological
The nature of the perinatal period to an important extent determines the developmental characteristics and health status of the fetus, as well as in childhood and adulthood. The course of the perinatal period of ontogenesis is significantly influenced by factors that determine the developmental features of the embryo and fetus before reaching 28 weeks, as well as the state of the parents’ reproductive cells (gametes), which gave rise to a new life. Modern science knows that developmental anomalies and diseases of the fetus are primarily caused by [1]:
- chromosomal and gene disorders (mutations);
- influence of unfavorable environmental factors;
- genetic disorders that can be realized (manifest) only as a result of exposure to unfavorable environmental factors.
Due to the fact that pathological factors influencing the risk of perinatal pathology have different effects, they are distinguished[1]:
- gametopathies;
- embryopathies;
- fetopathy.
| This section of the article has not been written. According to the plan of one or more Wikipedia contributors, a special section should be located in this place. You can help by writing this section. This mark was set on September 30, 2021 . |
Factors influencing the length of pregnancy
First of all, the duration of gestation is influenced by the health of the expectant mother and other factors . For example:
- heredity;
- psychological condition;
- fetal development;
- intrauterine condition.
In case of prematurity, as well as post-term pregnancy, there are additional threats of unfavorable birth , which can affect the health of the fetus and mother.
These phenomena may be caused by neuroendocrine disorders, previous diseases and previous abortions. According to statistics, women who have been treated for a threatened miscarriage are more likely to carry their fetus to term. A post-term pregnancy is considered to be one whose term has crossed the line of 42 weeks .
In this article you will find out: can pregnant women eat melon?
And here you can read an article about whether pregnant women can play sports.
Pregnancy against the background of extragenital pathology
In the structure of extragenital pathology (extragenital diseases) in pregnant women, the first place is occupied by pathology (diseases) of the cardiovascular system (80%), including congenital and acquired heart defects (including rheumatic heart defects), conditions after cardiac surgery, arterial hypertension, hypertension.
| This section of the article has not been written. According to the plan of one or more Wikipedia contributors, a special section should be located in this place. You can help by writing this section. This mark was set on September 30, 2021 . |
Complications of pregnancy
Pregnancy does not always go smoothly. Complications include:
- Nausea and excessive vomiting during pregnancy;
- Frozen pregnancy;
- Threat of miscarriage;
- Varicose veins of the lower extremities;
- Varicose veins of the vagina;
- Late toxicoses: nephropathy of pregnancy, preeclampsia and eclampsia;
- Fetal hypoxia;
- Lower back pain;
- Anemia (anemia) in the mother;
- Immunological conflicts and Rhesus conflict between mother and fetus;
- Fetoplacental insufficiency;
- Feto-fetal transfusion syndrome;
- Preeclampsia
A separate type of complicated pregnancy is ectopic pregnancy. In this case, fetal development is impossible, and sooner or later it ends in miscarriage.
In most cases, with timely detection, modern medicine is able to prevent and reduce undesirable consequences to a minimum.
Smoking and pregnancy
According to some data, maternal smoking increases the risk of newborn death by 20-35%[9]. According to other data, smoking increases the risk of death of a child in the first four weeks of his life by 40%[10]. Women who smoke are more likely than non-smokers to experience pathologies during pregnancy and childbirth[11].
Passive smoking also harms the pregnant woman and the fetus. Thus, non-smoking wives of smoking husbands are more likely than others to experience toxicosis in early and late pregnancy[12].
The effect of smoking at different stages of pregnancy[13]
| Term | Influence |
| 1st trimester | Dangerous, it occurs against the background of the formation of all the main organs of the human body. May lead to spontaneous miscarriage. There is a risk of fetal death. |
| 2nd trimester | Periodically aggravates toxicosis. The child develops worse and gains less weight. There is a risk of premature birth. |
| 3rd trimester | Dangerously, the likelihood of developing preeclampsia increases compared to the average. Negative infant mortality rates. |
Duration of pregnancy in women
How many weeks is pregnancy? It is very difficult to calculate the exact date of birth, and the day when the baby is due to be born is called in medical circles PDR - this is the expected date of birth.
It also happens when the expected date of birth coincides with the actual one, but you should not think that your gynecologist could accurately determine it. It was just a coincidence.
If the expectant mother knows the day when conception occurred and the day of ovulation, then it is impossible to determine the speed of the sperm and the number of days during which the egg can move through the fallopian tubes. Moreover, a woman cannot feel the implantation of the unborn baby to the wall of the uterus, which also affects the timing of pregnancy.
It is also worth paying attention to the fact that each woman’s pregnancy can proceed differently, therefore, experts use the average statistical standard, which is used when calculating the day of birth.
Almost all expectant mothers are interested in how many weeks a woman’s pregnancy lasts. For an answer to this question, you need to turn to scientists, who have calculated that in 80% of pregnant women, 266 days pass from the beginning of conception to the day of birth.
Therefore, we can conclude that on average, the duration of pregnancy is 38 weeks. But you should not rely on these statistics, because a huge number of pregnant women simply do not know on what day conception occurred.
The last menstruation is very helpful in calculating the day the baby was born, because every representative of the fairer sex probably remembers the last time they were. In this case, obstetricians start counting from the last menstrual period, which means that the pregnancy lasts 40 weeks.
Since fertilization did not occur on the first day of menstruation, forty weeks is an estimated period, called the menstrual or gestational period.
As for the fetus, its age is approximately two weeks younger than experts assume, therefore, if you pay attention to this, the gestational age will be more accurate, and its name will be ovulation or fertilization. In order to know the specific day of birth, you need to refer to the date of ovulation.
Preeclampsia
William Hunter, Anatomia uteri humani gravidi tabulis illustrata
, 1774
Gestosis is a complication of ongoing pregnancy, characterized by a disorder of organs and body systems.
It is believed that the pathogenesis is based on generalized vascular spasm and subsequent changes associated with impaired microcirculation, hypoperfusion, hypovolemia
Classification
Early gestosis: vomiting and uncontrollable vomiting (excessive vomiting), drooling.
Late gestosis: dropsy, nephropathy, preeclampsia, eclampsia.
Rare forms of gestosis: diseases of the skin, liver (jaundice of pregnant women), nervous, bone and other systems.
Also distinguished:
- “pure” gestosis - occurring in the absence of background diseases, in the midst of complete health.
- “combined” gestosis arising on the basis of a previous disease (hypertension, kidney disease, endocrinopathies).
Etiology and pathogenesis
Currently, there is no consensus on the etiology of gestosis. However, there are a number of theories:
The cortico-visceral theory is based on the idea of gestosis as a kind of neurosis of pregnant women, in which the relationship between the cortex and subcortical structures is disrupted. This leads to reflex changes in hemodynamics. This theory is confirmed by the frequent occurrence of gestosis in pregnant women against the background of neuropsychic stress. EEG reveals functional changes in subcortical structures.
Endocrine theory.
The immunological theory is to change the mechanisms that provide transplacental immunity. The essence of the theory is that the placenta produces a number of substances that block the mother's T cells. The process of T-cell recognition of antigenic differences between maternal and fetal tissues is disrupted, which leads to sensitization of the mother by placental proteins. The antigenic structure of the placenta is similar to the tissues of the kidneys and liver, which can cause damage to these organs during gestosis. However, not all scientists found immune complexes in the mother’s blood.
Genetic theory - it was found that in the daughters of women with preeclampsia, gestosis occurred 8 times more often than in the normal population. An autosomal recessive mode of inheritance has been suggested.
The theory of vitamin B deficiency and folic acid. [ source not specified 1805 days
].
In the third trimester, the need for B vitamins and folic acid increases. The intake of these vitamins from the daily diet becomes insufficient. As a result, the concentration of homocysteine in the blood increases. [source not specified 655 days] Homocysteine is extremely toxic to the endothelium. Under its influence, pores appear in the vascular endothelium through which plasma escapes into the surrounding tissues. Swelling occurs. In response to a decrease in blood volume, the pituitary gland releases vasopressin, which increases pressure in the blood vessels and reduces diuresis. This theory is confirmed by practice, since the administration of B vitamins and folic acid in large doses to women with gestosis throughout the day leads to the disappearance of edema, normalization of blood pressure and cessation of proteinuria. [ source not specified 1805 days
].
Placental theory. Probably, in women suffering from gestosis, the migration of trophoblast into the vessels of the uterus is impaired. The spiral uterine arteries do not change their structure and remain in the same form as in non-pregnant women. The relationship in the trophoblast-spiral artery system is disrupted, spasm occurs, decreased intervillous blood flow and hypoxia occur. Hypoxia in the tissues of the uteroplacental complex leads to damage to the endothelium, disruption of its vasoactive properties, and the release of mediators aimed at vasoconstriction. Long-term production of vasoconstrictors causes disturbances in hemodynamics, the central nervous system, hormonal status, metabolism and acid-base balance of the body.
The pathogenesis is based on generalized vasospasm, which is manifested by hypertension. The spasm occurs due to damage to the endothelium. (Damage to the endothelium is confirmed by an increase in the blood level of fibronectin, a glycoprotein of subendothelial origin.) When damaged, endothelin is released into the blood, which leads to spasm of blood vessels, including the renal arteries and activation of the renin-angiotensin-aldosterone system, as well as the release of adrenaline and norepinephrine and reducing the threshold of sensitivity to these mediators.
At the same time, the synthesis of vasodilators decreases.
Due to vasospasm, hypoxia, and a decrease in the anticoagulant properties of the blood, hypercoagulation and disseminated intravascular coagulation develop [ source not specified 1805 days
]. Microcirculation is also disrupted, the permeability of the microvascular bed increases, and plasma sweats into the interstitium (which leads to edema with a decrease in blood volume).
Hypoxic (dystrophic) changes occur in many organs: gestosis is almost always accompanied by impaired renal function, the function of the liver, nervous system, and placenta is impaired. Fetal growth retardation syndrome and chronic hypoxia occur.
Clinical picture
Early gestosis
Vomiting and uncontrollable vomiting in pregnancy.
Preeclampsia includes vomiting during pregnancy, which occurs not only in the morning, but also repeats several times a day, even after eating. Nausea accompanied by vomiting, appetite usually decreases, and a tendency to eat spicy and salty foods appears. Despite vomiting, a significant decrease in the pregnant woman’s body weight is not observed. Pregnant women complain of weakness, irritability, drowsiness, and sometimes insomnia. The general condition is satisfactory, the temperature is normal, the pulse can be up to 90 beats. per minute Vomiting occurs during the first 2-3 months of pregnancy, is easily treated or goes away spontaneously. Only in some women does vomiting intensify and acquire the character of uncontrollable vomiting. It is believed that when carrying the first child, early gestosis is more pronounced.
Uncontrollable vomiting.
Vomiting occurs 20 or more times a day; it happens day and night. A woman's body weight drops. There is a sharp weight loss, the subcutaneous fat layer disappears. The skin becomes flabby and dry, the tongue is coated, and there is an unpleasant odor from the mouth. An aversion to food appears. The temperature is low-grade, the pulse is up to 100-120 beats per minute, blood pressure drops, acetone and protein appear in the urine. In particularly severe cases, a high temperature, icteric discoloration of the skin, a sharp increase in heart rate and arrhythmia are observed, and a delirious state may develop.
Salivation.
It is often observed with vomiting of pregnant women, but can manifest itself in the form of independent gestosis. The amount of saliva produced can reach 1 liter. The pregnant woman’s health worsens, insomnia occurs, and her body weight decreases.
Late gestosis
Late gestosis represents stages in the development of a single pathological process. The initial form is dropsy, which progresses to a more severe form - nephropathy, which progresses successively to preeclampsia and eclampsia.
see also
- Pregnancy in animals
- Twins
- Preeclampsia
- Movement "For Life"
- Diabetes in pregnancy
- Human conception
- Birth control
- Immunobiology of pregnancy
- Induced abortion
- Multiple pregnancy
- Maternity leave
- Signs of pregnancy
- Reproductive health
- Childbirth
- Superfetation
- Contractions
- The course of pregnancy in humans
- Adoption
- Embryology
Notes
- ↑ 1 2 3 4 5 Vikhlyaeva E. M., Kulakov V. I., Serov V. N. et al. Ed.
G. M. Savelyeva. Handbook of obstetrics and gynecology. — 1st ed. - M.: Medicine, 1992. - P. 8-108. — 352 p. — (Reference publication). — 50,000 copies. — ISBN 5-225-02599-4. - O. OSKOLKOVA Family planning in developing countries of Asia
- G. M. Savelyeva
Obstetrics. Textbook for medical universities, p. 98 - E.K. Aylamazyan
Obstetrics. Textbook for medical schools, chapter 9. - 3D Pregnancy Archived September 27, 2007. (Image from gestational age of 6 weeks). Retrieved 2007-08-28. A rotatable 3D version of this photo is available here Archived September 14, 2007, and a sketch is available here Archived September 27, 2007.
- 3D Pregnancy Archived September 27, 2007. (Image from gestational age of 10 weeks). Retrieved 2007-08-28. A rotatable 3D version of this photo is available here Archived September 16, 2007, and a sketch is available here Archived September 27, 2007.
- 3D Pregnancy Archived September 27, 2007. (Image from gestational age of 20 weeks). Retrieved 2007-08-28. A rotatable 3D version of this photo is available here Archived September 16, 2007, and a sketch is available here Archived September 27, 2007.
- 3D Pregnancy Archived September 27, 2007. (Image from gestational age of 40 weeks). Retrieved 2007-08-28. A rotatable 3D version of this photo is available here Archived September 16, 2007, and a sketch is available here Archived September 27, 2007.
- Mannino D., Klevens MR & Flander DW (1994) Cigarette smoking: an independent risk factor for impotence. American Journal of Epidemiology 140: 1003-8
- British Medical Association (2004) Smoking and reproductive life: The impact of smoking on sexual, reproductive and child health. London. B.M.A.
- Domain osgm.ru maybe for sale Archived September 24, 2015.
- Dangers of secondhand smoke for a pregnant woman
- Can pregnant women smoke? (Russian), Children's website Babies info
(June 2, 2017). Retrieved June 6, 2021.
Literature
- Pregnancy // Encyclopedic Dictionary of Brockhaus and Efron: in 86 volumes (82 volumes and 4 additional). - St. Petersburg, 1890-1907.
- Joanna Stone, Keith Eddleman, Mary Murray.
Pregnancy for dummies = Pregnancy For Dummies. - M.: "Dialectics", 2010. - P. 272. - ISBN 978-5-8459-1690-7. - Kovalenko N.P.Professor, Doctor of Psychological Sciences.
“On the Good Path to a Successful Childbirth” = “On the Good Path to a Successful Childbirth.” - M. - Kovalenko N.P.Professor, Doctor of Psychological Sciences.
"Psychoprophylaxis and psychocorrection during pregnancy and childbirth." - M. - Kovalenko N.P.Professor, Doctor of Psychological Sciences.
"Perinatal psychology". - M. - Kovalenko N.P.Professor, Doctor of Psychological Sciences.
“Scientific collection on perinatal psychology of the Russian Association of Perinatal Psychology and Medicine from 2001-2008” (annually) edited by Kovalenko N.P. - M. - Katherine Crum, Teri Stuffer Drenth.
Physical education during pregnancy for dummies = Fit Pregnancy For Dummies. - M.: “Dialectics”, 2007. - P. 362. - ISBN 0-7645-5829-3. - G. M. Savelyeva, V. I. Kulakov.
Obstetrics. - M.: Medicine, 2000. - P. 816. - ISBN 5-225-04549-9. - V.E.
Radzinsky. Early pregnancy. - M.: Media Bureau Status Present, 2009. - P. 479. - ISBN 978-5-91785-001-6.