What is the best position for my baby to give birth?
Labor is almost always faster and easier if your baby is in a head-down position with the back of his head facing your belly. This position of the fetus is called “cephalic presentation, anterior view.” In most cases, the baby takes exactly this position by the end of pregnancy. Being in the forward position, the baby is most comfortable in the curve of your womb. During labor, the baby tilts his head forward so that his chin touches his chest. In this position, childbirth proceeds easier and faster, because in this case:
- During contractions, the crown of the baby puts gentle and even pressure on the cervix. This promotes the dilation of the cervix and the release of hormones necessary for the successful course of labor.
- During pushing, the child passes through the pelvic bones at an angle at which the smallest circumference of his head is in front. To better visualize this, try wearing a shirt with a tight-fitting high collar, without hiding your chin, and everything will immediately become clear to you.
- When the baby reaches the pelvic floor, he turns his head slightly so that the widest part of it is in the widest part of the pelvis. In this case, the back of his head may pass under your pubic bone. When born, the baby leaves the mother's body, sliding his face along the surface located between the vagina and the anus (perineum).
How to determine the transverse position of the fetus
To determine the incorrect position of the fetus, a comprehensive examination of the pregnant woman is carried out:
Abdominal examination
During examination of a pregnant woman's abdomen, its irregular shape is revealed. The abdomen is stretched transversely when the fetus is transversely positioned or has an obliquely stretched shape in the case of an oblique position of the baby. The uterus takes the shape of a ball instead of the ovoid-elongated one. When measuring the size of the abdomen, it is established that its circumference significantly exceeds the norm, although the height of the uterine fundus does not coincide with the gestational age (smaller).
Palpation of the abdomen
During palpation of the abdomen, it is impossible to determine the presenting (large part of the fetus) part at the entrance to the bony ring of the pelvis. The head or pelvic end is also not palpable in the fundus of the uterus. Large parts of the baby can be felt on the right or left side of the midline of the uterus. The position of the fetus is determined by the head. If the head is on the left, we speak of the first position, if the head is located on the right, we speak of the second. The fetal heartbeat can be heard well in the navel area, and not on the left or right, as in the longitudinal position. It may be difficult to establish the position and position of the baby in case of uterine hypertonicity (threat of premature birth) and in case of excess amniotic fluid.
Obstetric ultrasound
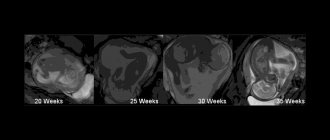
Obstetric ultrasound with a 100% guarantee determines the position of the fetus at any stage of gestation. But, as already mentioned, the transverse position of the baby at 20 weeks should not be a reason for panic; before the due date of birth, the fetus will have time to take the “correct” position.
Vaginal examination
A vaginal examination, which is performed at the end of pregnancy or when contractions have begun but the amniotic sac is intact, provides little information. The obstetrician can only determine that the presenting part of the fetus at the entrance to the pelvis is missing. In the case of rupture of water and the opening of the uterine pharynx to 4 cm or more, a vaginal examination is carried out with caution, as it can provoke prolapse of the arm, fetal leg or umbilical cord loop. If the water has leaked, the doctor can feel the side of the fetus (ribs with intercostal spaces), the shoulder blade or armpit, and in some cases the elbow or hand.
What is back position?
The posterior position is a position in which your baby's head is down and the back of his head is facing your spine. By the time labor begins, approximately every tenth child is in this position. In most cases, these babies are born during a normal, vaginal birth, but this placement creates additional difficulties for the mother, especially if the baby's chin is raised up instead of down. As a result:
- you may experience lower back pain caused by the pressure of the baby's head on your spine,
- your water may break early,
- labor can be long and slow,
- you may begin to feel pushing before your cervix is fully dilated.
When the baby reaches the pelvic floor, he will have to turn almost 180 degrees in order to get into the position most comfortable for birth. This process may take some time, and it also happens that the child prefers not to roll over at all! In the latter case, he is born face up, as if looking at you. In addition, in this case, to help it be born, you may need forceps or a vacuum extractor.
Why do some children take a back position?
If your baby is in a posterior position, it may be due to the type and shape of your pelvis. The female pelvis is sometimes not round, but rather narrow, oval-shaped (the so-called anthropoid pelvis) or wide, heart-shaped (the so-called android pelvis or male-type pelvis). If your pelvis is not round but oval or heart-shaped, then there is a relatively high chance that your baby will take a back-to-back position at the widest part of your pelvis. The fact is that in this position it is easier for him to support his head. The mother's lifestyle also plays a role. It appears that posterior fetal position is much more common among European women than among women in developing countries, who are accustomed to working in the fields all day and eating or preparing food while squatting. The reason is quite obvious. When you watch TV, sitting comfortably in a chair, or work for hours at a computer, your pelvis is tilted back. In this case, naturally, the heaviest part of the child’s body (the back of the head and spine) also tends to lean back. So, in the end, the child ends up in a back-to-back position. If you work a lot or spend time standing, your baby will most likely take an anterior position in the pelvic cavity because your pelvis is always tilted forward.
Position of fetuses in twins
With twins, vaginal delivery is possible if both fetuses are in the cephalic presentation, or if the first (which is closer to the exit from the uterus and will be born first) is in the cephalic presentation, and the second in the breech. If, on the contrary, the first is in a breech presentation, and the second is in a cephalic presentation, the situation is unfavorable, since after the birth of the pelvic end of the first fetus, the babies can get their heads caught.
When determining the transverse position of one of the fetuses, the issue is resolved in favor of a cesarean section.
Even with a favorable position of the fetuses, the question of the method of delivery for twins is decided not only based on the position, but also depending on many other factors.
How can I help my child get into a forward position?
You may have heard about so-called methods to give the fetus an optimal position. These are techniques that can help your baby achieve a forward position by changing your posture, especially when sitting. Remember: you want your pelvis to tilt forward, not backward. Therefore, when you sit, make sure that your knees are always lower than your hips. Try the following:
- Pay attention to the design of your favorite chair. It should not be such that your knees rise above your hips when you sit down. If this happens, try turning the chair 180 degrees, kneeling on the seat and leaning forward, leaning over the back.
- Clean the floors. Our grandmothers liked to repeat that cleaning the kitchen floor is the best way to prepare for childbirth. And they were right! While you are on all fours, your baby turns the back of his head towards your stomach.
- When driving a car, place a pillow on the seat so that your pelvis is elevated in relation to your legs.
- While sitting in front of the TV, lean forward, leaning over the fitball.
When you go to bed, you don't have to worry about your baby's position. However, the optimal sleeping position in late pregnancy is lying on your side, not on your back.
Let's define the terminology
Depending on how the fetus is located in the uterus, the woman’s delivery tactics are determined. To understand the terms, let’s define the following concepts:
- fetal axis – a longitudinal line connecting the buttocks and the baby’s head;
- uterine axis - a longitudinal line connecting the fundus of the uterus and the cervix, or the length of the uterus.
The position of the fetus is the relationship between the baby's axis and the length of the uterus. There is a difference between correct and incorrect fetal position. The correct position is considered to be longitudinal, when the axes of the uterus and the baby coincide, or simply, when the baby and the mother’s torso are in the same direction (if the mother is standing, then the baby is positioned vertically with her). In this case, one of the large (head or pelvic end) parts of the baby “looks” at the entrance of the small pelvis, and the other rests on the uterine fundus.
Incorrect positions are considered to be transverse and oblique positions of the fetus. But it should be remembered that the fetus is very mobile during most of pregnancy and constantly changes its position. Stabilization of its position occurs by 34 weeks, so talking about an incorrect position before the specified period does not make much sense.
Transverse position
In the case of the transverse position (situs transverses) of the child, it is located not along, but across the uterus, that is, the uterine axis and the axis of the fetus are perpendicular to each other and make an angle of 90 degrees. Since the baby is located transversely, there is, accordingly, no presenting part - large parts of the fetus can be felt on the sides of the uterus on the right and left and are located above the iliac crests.
What is called an oblique position?
The oblique position of the fetus (situs obliguus) is said to occur when the axis of the fetus is displaced relative to the length of the uterus, which forms an acute angle (less than 45 degrees). In this case, the head or buttocks are located below the iliac crest. You can also distinguish the transverse oblique position (does not play a big role), when the axes of the fetus and uterus are located at an angle, but do not reach 90 degrees, but more than 45 degrees.
It is also worth mentioning the unstable position of the fetus. With significant mobility of the fetus, it periodically changes its position from longitudinal to transverse or oblique and vice versa.
Fetal presentation
The presentation of the fetus is the relationship of its large part (this can be the head or pelvic end) to the entrance to the pelvis. Accordingly, a distinction is made between cephalic presentation (the head is located at the entrance to the small pelvis) and pelvic presentation (can be leg, breech or mixed).
Will I actually be able to get my baby into the correct prenatal position?
Trying to bring a baby into the correct prenatal position is a long-known practice; there is nothing particularly new here. The first reports of “giving the fetus an optimal position” appeared in the 19th century. Today this method is known thanks to a description proposed by obstetrician Jean Sutton and published in the 1990s. Jean Sutton suggested that women in late pregnancy adopt an upright or forward-leaning position as often as possible. One often hears the question: does this really help, or does it simply create additional difficulties for a pregnant woman? So far, research on this method only confirms that in late pregnancy, staying in the knee-elbow position twice a day for 10 minutes really helps the baby take a forward position. Unfortunately, this does not seem to affect the position of the baby during birth. As for getting into an upright or forward-leaning position, Sutton recommends doing this regularly. If you practice the described technique during pregnancy, but despite this, the baby ends up in a posterior position when labor begins, this may be explained more by the shape of your pelvis than by your posture.