For proper growth and development, it is extremely important for a child’s body to receive the required amount of vitamins, minerals and trace elements. A deficiency of a certain microelement can significantly affect the child’s health and also lead to the development of anemia. This especially applies to the lack of the nutrient iron in the body. Its main functional task is oxygen supply to all tissues. This is why it is so important to monitor blood counts from time to time in order to promptly identify possible iron deficiency anemia.
Causes of iron deficiency in childhood
Obvious iron deficiency in a child’s body can develop in situations where its intake is lower than its consumption. The causes of iron deficiency in childhood can be:
- Poor nutrition of the child (vegetarianism, fasting).
- Vitamin C deficiency.
- Violation of absorption processes in the intestines.
- Excessive dietary intake of oxalates, calcium, vitamin E and zinc, which block the absorption of iron.
- Chronic lead poisoning or overuse of antacids.
- Increased iron consumption during periods of intensive growth.
- Thyroid gland dysfunction.
- Injuries with heavy bleeding, surgical interventions.
- Reduced acid-forming function of the stomach.
- Worm infestation.
- Tumor formations and systemic diseases.
A common cause of iron deficiency can be acute blood loss in children as a result of intussusception and abdominal injuries of various locations. In the first year of life, anemia in a child is associated with low iron content in the mother's breast milk.
With a long-term lack of iron in the child’s body, its reserves gradually run out - iron deficiency anemia develops. Its main signs are a decrease in hemoglobin in a general blood test, a decrease in the level of the color index, and the appearance of atypical red blood cells with different shapes, sizes and colors.
Signs of iron deficiency in a child
There are established iron requirements for each age group, which children should, if possible, receive every day (the established amount is a guideline, but ignoring enough iron can lead to serious consequences):
- Seven months to one year – 11 milligrams.
- One to three years – 7 milligrams.
- From four to eight years – 10 milligrams.
- From nine to thirteen years – 8 milligrams.
If you do not consume the prescribed amount of iron, then symptoms of iron deficiency in the child's body will appear. Critically low iron levels have a significant impact on functional ability. Insufficient levels of an important microelement are divided into several stages, which may not appear during a blood test, but the child will show some external signs.
Most of the symptoms of iron deficiency in the body in children may not manifest themselves at all, exactly until the moment when the presence of iron deficiency anemia is diagnosed. Then this pathological condition will manifest itself with the following symptoms: increased fatigue, weakness throughout the body, pallor of the skin, disruption of the structure of hair and nails, loss of appetite, irritability and shortness of breath.
The most common and main symptoms of iron deficiency in a child are weakness, drowsiness and apathy. Also quite often, children experience severe headaches, a feeling of numbness in their fingers, the appearance of “spots” in the eyes, and cases of dizziness or loss of consciousness. Children with insufficient levels of iron in the body are susceptible to the appearance of an infectious disease, they develop eating disorders, inflammation of the tongue, and the appearance of cracks around the mouth.
Symptoms of iron deficiency anemia
The first symptoms of iron deficiency anemia are general weakness and fatigue.
General weakness comes to the fore among complaints with the development of anemic syndrome in patients. With long-term iron deficiency, the functioning of all organs and systems, including the brain, suffers, so children often complain of fatigue, become drowsy and irritable. Often there are flashing spots before the eyes, loss of consciousness, headache, and numbness of the limbs.
In advanced cases of the disease, shortness of breath appears even with minimal physical exertion, appetite worsens or its perversion occurs: the use of substances that do not have nutritional value (chalk, earth, metal objects).
When examining a child, you can reveal pale and dry skin, cracks in the corners of the mouth, smoothness of the papillae of the tongue, striations and defects on the nail plates. A mild degree of iron deficiency is manifested by rapid fatigue, headache, memory impairment, decreased academic performance in schoolchildren and decreased immunity.
Normal iron levels
The amount of iron at different periods of a child’s life varies depending on gender and age needs. The average daily dose in children is:
- from birth to 1 year – from 4 to 10 mg;
- after the age of 1 year and up to 6 years – 10 mg;
- from 6 to 10 years – no more than 12 mg;
- for boys from 11 to 17 years old - 15 mg, for girls - 18 mg.
In the first year of life, especially up to 2 months, most children's need for iron increases sharply. This is due to the complete replacement of fetal red blood cells with normal ones after birth. And during the period of intensive growth and puberty, iron consumption in the child’s body increases sharply, especially in girls during the formation of the menstrual cycle.
Children's bodies best absorb II valence iron in the presence of ascorbic acid. A microelement with this valence is found only in medicines. The products deliver III-valent iron, which turns into II-valent iron in the body.
The diagnosis of “mild anemia” can be made when the hemoglobin level is below 100 g/l, when the level drops below 90 g/l - moderate, and below 70 g/l - severe.
Why is iron deficiency dangerous in children?
Doctors have known about the importance of a balanced diet and adherence to nutrition for a long time. In contrast to the serious approach to feeding children in the first year of life, relatively little attention is paid to the nutrition of children over one year of age, despite the fact that a balanced diet remains very important at the stage of rapid growth and development of the child’s body at any age.
The formation of eating behavior that occurs in childhood remains very important Individual taste preferences arise both on a genetic basis and on the basis of previous experience. Recent studies have shown that children prefer fruits and vegetables that have greater energy potential (more calories per gram). The innate preference for sweet, energy-dense foods, the desire or reluctance to eat anything in young children can become a serious obstacle to ensuring a complete and balanced diet. The nature of nutrition changes rapidly in the period from 9 months to 3 years, as the child switches to the diet accepted in the family. The culture of feeding children directly depends on the eating behavior of parents. The modern rhythm and socio-economic factors have a significant impact on the lifestyle and nutrition of an adult:
- Women going to work soon after giving birth to support the family budget reduces the time previously devoted to the child.
- The lack of a culture of “family dinners” leads to scattered meals and non-compliance with the diet.
- Convenience is becoming more and more important, so fast food, snacks, and convenience foods are consumed in greater quantities.
- Young children often eat outside the home, so parents pay more attention to the convenience of food packaging than to the contents.
As a result of the influences of modern lifestyle, the nature of nutrition of children of the younger age group and preschoolers has changed significantly. Several studies conducted in Russia in recent years have shown that the diet of children in the younger age group is far from ideal:
- 72% of children eat glazed cheese curds or sweet yoghurts for breakfast;
- every tenth child does not eat fruit;
- some children drink about 1100 ml/day of cow's milk;
- 17% of children do not eat meat at all;
- Only 52% of children eat fish.
These studies clearly demonstrated an imbalance in the diet of children in the younger age group in Russia. The general picture obtained as a result of these studies requires no comment.
Considering the nature of nutrition of young children in Russia today and the lack of balance of its elements, children are susceptible to developing deficiencies or excesses of any nutrients, which may become a problem for their health in the future. Thus, for infants and young children, the amount of iron required is equal to the needs of an adult man (on average 10 mg/day), and per kilogram of body weight, a child needs 5 times more iron daily than an adult. Consequently, an unbalanced diet at this age is critical - even minor deviations in the diet lead to the development of deficiency conditions.
Iron deficiency... According to Russian data, more than 40% of young children have iron deficiency anemia. Taking into account that iron deficiency conditions without anemia are 1.5–2 times more common, it can be assumed that more than 60% of young children in Russia suffer from iron deficiency. Despite the relative ease of diagnosis and treatment, iron deficiency remains a major health problem worldwide. According to WHO, iron deficiency occurs in almost 30% of the world's population, and in some risk groups, particularly in children 5-14 years old, its incidence reaches an alarming 82%.
Manifestations of iron deficiency are different: the most common manifestation is the development of iron deficiency anemia , also among the manifestations there may be signs of damage to epithelial tissue - roughness, dry skin, angular stomatitis, cheilitis, glossitis or atrophy of the oral mucosa, fragility and dullness of hair, hair loss, dullness and brittleness of nails, tooth decay (caries). Headaches and dizziness, weakness, fatigue, cold intolerance, decreased memory and concentration, slowed mental and physical development in children, inappropriate behavior; rapid heartbeat with little physical activity, cracking of the mucous membranes in the corners of the mouth, redness and smoothness of the surface of the tongue, atrophy of the taste buds; fragility, thinning, deformation of nails; perversion of taste (craving for eating non-food substances), especially in young children, difficulty swallowing, constipation; inhibition of cellular and humoral immunity; increased general morbidity (colds and infectious diseases in children, pustular skin lesions, pathological changes in the intestinal epithelium with impaired intestinal absorption; increased risk of developing tumor diseases.
Due to the participation of iron in the construction of certain brain structures, its deficiency in the prenatal period and in children of the first two years of life can lead to learning and behavioral disorders. Iron deficiency in the fetus, and subsequently in young children, can lead to impaired mental development, hyperexcitability in combination with inattention syndrome, poor cognitive function and delayed psychomotor development, due to functional failure of myocytes (muscle cells) and slower myelination of nerve fibers. Children and adolescents with iron deficiency develop pathological changes in the intestinal epithelium with impaired intestinal absorption, which is often accompanied by poor hair and nail growth. In adolescents, iron deficiency leads to impaired memory and social behavior, and decreased intellectual capabilities. Iron deficiency can also cause other health problems in children.
It is generally accepted that preventive measures can prevent the development of iron deficiency conditions. It is necessary to provide the child's diet with the main sources of iron (red meat, offal, fish, eggs, etc.), it is important to take into account the bioavailability of iron in the diet - control the amount of consumption of foods low in iron and foods that interfere with the absorption of iron.
The main sources of iron are: cereals, liver, meat. Children under one year old absorb up to 70% of the iron in food, children under 10 years old - 10%, adults - 3%. The mechanisms of regulation of iron absorption have not been fully elucidated, but it has been established that absorption accelerates with iron deficiency and slows down with an increase in its reserves in the body. The body regulates iron stores depending on its needs by increasing its absorption at the same amount. Calcium, vitamins C, B12, gastric acid, pepsin, and copper promote the absorption of iron, especially if they come from animal sources. Phosphates contained in eggs, cheese and milk, oxalates, phytates and tannins contained in black tea, bran, and coffee interfere with the absorption of iron. A decrease in gastric acidity as a result of prolonged use of antacids or drugs to reduce acidity is also accompanied by a decrease in iron absorption.
Based on the above, we can identify the main causes of iron deficiency in children:
- insufficient intake (inadequate nutrition, vegetarian diet, malnutrition and other types of altered eating behavior in the family);
- decreased absorption of iron in the intestines;
- dysregulation of vitamin C metabolism;
- excessive intake of phosphates, oxalates, calcium, zinc, vitamin E into the body;
- entry into the body of iron-binding substances (complexones);
- lead poisoning, antacids;
- increased consumption of iron (during periods of intensive growth and pregnancy);
- iron loss associated with injuries, blood loss during operations, heavy menstruation, peptic ulcers, donation, and sports;
- hormonal disorders (thyroid dysfunction);
- gastritis with reduced acid-forming function, dysbacteriosis;
- various severe infectious, systemic and tumor diseases;
- helminthic infestation.
Treatment of anemia in children should be comprehensive and based on normalizing the child’s diet and diet, possible correction of the cause of iron deficiency, prescribing iron supplements, and concomitant therapy.
Iron preparations are usually prescribed orally, and only for diseases accompanied by malabsorption or severe side effects, intramuscular or intravenous injections of drugs are indicated. The duration of treatment is from 4 to 7 months, depending on the severity of anemia. Such long-term treatment is necessary because restoration of iron stores occurs slowly, after normalization of hemoglobin levels. The daily dose of iron supplements is selected according to the weight and age of the child and the severity of iron deficiency.
Evaluation of the effectiveness of the therapy is possible by the 10th day from the start of treatment. And restoration of hemoglobin levels in mild to moderate anemia is possible already by the third week of therapy.
Currently, the pharmaceutical industry produces a fairly large number of iron preparations and the development of new drugs continues. There was a need to classify iron preparations and describe their properties in order to facilitate the choice. Depending on the method of administration to the body, iron preparations are divided into oral and parenteral (intravenous, intramuscular).
For many years, the gold standard for oral iron supplements was ferrous sulfate. The latter is an iron salt preparation, which is inexpensive to produce and, accordingly, has a low cost. For this reason, a large number of iron preparations containing ferrous sulfate are currently produced (Aktiferrin, Hemofer prolongatum, Sorbifer Durules, Tardiferon, Ferroplex, Ferrogradumet, Ferro-Folgamma, etc.).
But when using iron salt preparations, local irritation of the gastric mucosa at the site of dissolution of the drug and the mucous membrane of the duodenum, where the drug is predominantly absorbed, is possible. Due to their low molecular weight, iron salt preparations can be absorbed in large quantities, leading to dangerous concentrations for the body, which can cause intoxication and poisoning.
During the treatment of IDA with iron salt preparations, the following problems may arise:
- poor tolerability due to toxicity mainly for the gastrointestinal tract (stomach pain, nausea, vomiting, constipation, diarrhea), which forces the use of iron salt preparations in low doses (3 mg/kg per day);
- possible interaction with other drugs, which requires studying the instructions for all drugs used in a particular patient;
- interaction with food, since there are products that reduce (tannin, caffeine, large amounts of protein) and increase (ascorbic acid, acidic juices) the absorption of iron salt preparations;
- pronounced metallic taste;
- staining of the enamel of teeth and gums, sometimes permanent;
- the possibility of overdose and poisoning due to passive, uncontrolled by the body absorption of a substance with a low molecular weight. Poisoning with iron salt preparations accounts for only 1.6% of all cases of poisoning in children, but in 41.2% of cases they are fatal;
- frequent refusal of treatment by patients, low feasibility of treatment (compliance): 30–35% or more of children and pregnant women who started treatment soon stop it.
In order to overcome the above-mentioned negative properties of iron salt preparations and, above all, improve tolerability, an iron preparation based on polymaltose hydroxide complex (HPC) was created. The features of these iron preparations are: the presence of a ferric iron nucleus in the central part of the complex. Today, a doctor’s arsenal includes modern ferric iron preparations based on various polysaccharide complexes: oral iron preparations based on HPA (Maltofer, Maltofer Fol, Ferrum Lek); iron preparations based on CGP (Ferrum Lek - solution for intramuscular administration); iron preparations based on hydroxide sucrose complex (Venofer - solution for intravenous administration); iron preparations based on carboxymaltose (Ferinject) and others.
Iron preparations based on HPA have the following properties and advantages over iron salt preparations:
- high efficiency;
- high safety, no risk of overdose, intoxication and poisoning;
- gums and teeth do not darken;
- the drugs have a pleasant taste;
- excellent tolerability, which determines the regularity of taking the drug;
- there is no interaction with other drugs and food;
- drugs have antioxidant properties;
- dosage forms have been developed for all age groups of patients (chewable tablets, drops, syrup, tablets).
Ferric iron preparations are leaders in modern pediatrics and are used with good effect in children of all age groups, even in children in the first months of life...
Be healthy!
- Author - Polukhina Anastasia Aleksandrovna
- 01.03.2016
- All consultations by the author
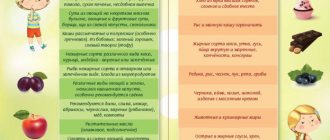
Food Sources of Iron
The main rule for correcting obvious or hidden iron deficiency is proper nutrition for the child, and for long-term anemia - pharmaceuticals and multivitamins. The diet of a child with iron deficiency anemia must include the following foods:
- liver;
- turkey or rabbit meat;
- beef tongue;
- peaches, apricots, apples, blueberries;
- legumes (peas, beans);
- cereals (buckwheat, oatmeal);
- bread (wheat, rye);
- seafood.
There are certain restrictions on the consumption of tea and coffee, which contain tannins that reduce the absorption of iron in the digestive tract. If necessary, iron-containing preparations can be washed down with purified water with the addition of lemon juice, which improves the absorption of the microelement.
When receiving iron in the form of a finished product, it is necessary to constantly monitor its level in the blood, since its excess can lead to a lot of complications.
Symptoms of iron poisoning include:
- Headache.
- A sharp decrease in appetite.
- Nausea, vomiting.
- Diarrhea.
- Dizziness.
- Reduced blood pressure levels.
- Inflammatory changes in the kidneys.
With the simultaneous use of iron in a dose of 900 mg or more, death can occur, so the drugs must be kept away from the baby’s eyes.
How to eliminate iron deficiency in a child
What needs to be done if the attending physician comes to the conclusion that the child has low iron in the blood? Low iron in a child’s blood can be eliminated by many methods, the main of which will be taking vitamin supplements and properly adjusting the diet. It is extremely important to prevent latent iron deficiency in children from developing into a pathological condition - iron deficiency anemia.
If a child has low iron in the red component of the body, then it is necessary to begin restorative treatment therapy. The attending physician may prescribe iron-containing medications if there is a critical shortage of this microelement. In other cases, it will be enough to make some adjustments to your diet and lifestyle. The iron found in breast milk is absorbed by the child's body much better than that found in formula. In the absence of breastfeeding, it would be advisable to use formulas that are fortified with iron.
The use of drugs that contain iron is necessary if the child was born much earlier than expected or with a very low weight, or if the mother stopped feeding the child breast milk, and after that the child did not receive foods high in the required substance for a long time . In these cases, the pediatrician may recommend taking iron supplements.
Also, we must not forget about products that help increase the absorption of essential microelements. Vitamin C and foods high in vitamin C are great for improving iron absorption. It is worth making some changes to the child’s diet and adding the following products: animal liver, rabbit meat, beef tongue, red fruits, peas and beans, buckwheat and oatmeal, seafood. Drug therapy includes taking iron and substances that enhance the absorption of this element.
Drug correction of anemia
For the treatment of iron deficiency anemia, iron single preparations or their combination with substances that enhance the absorption of the microelement in the intestine are widely used. There are two types of products on the pharmaceutical market for children - divalent and trivalent iron.
Prominent representatives of drugs for the treatment of anemia in childhood are: Aktiferrin, Ferrum Lek, Ferumbo, Hemofer, Maltofer. Each of them has its own advantages and disadvantages. The doctor should select the optimal drug for treating a child and set its dosage after a comprehensive examination.
Iron deficiency in a child’s body can cause many problems with its development, so parents need to take a serious approach to eliminating it. Treatment of iron deficiency should be comprehensive and include not only iron supplements, but also good nutrition, vitamin therapy, and walks in the fresh air.